Kala Azar in India – Symptoms, Treatment, Efforts
From Current Affairs Notes for UPSC » Editorials & In-depths » This topic
IAS EXPRESS Vs UPSC Prelims 2024: 85+ questions reflected
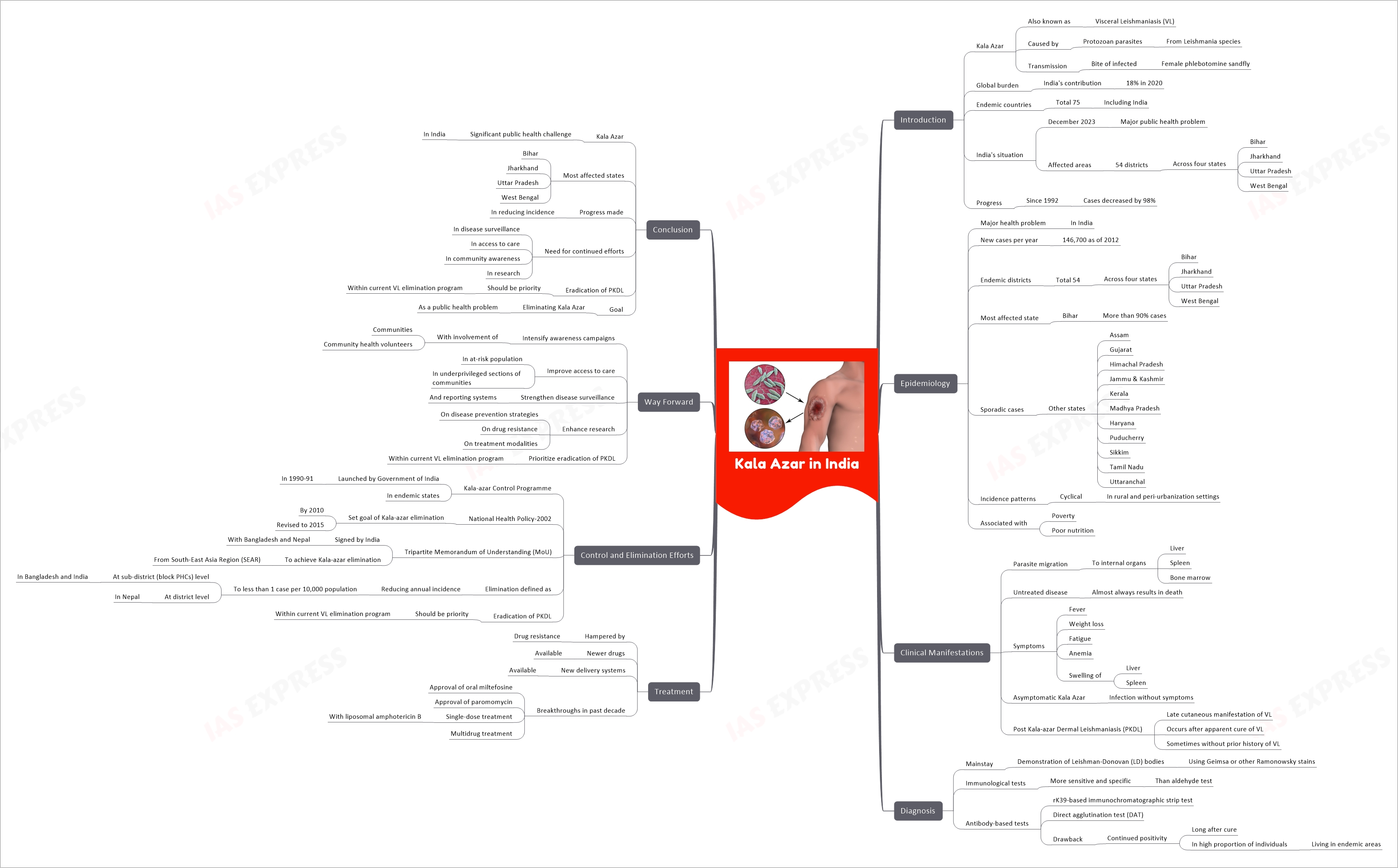
Kala Azar, also known as Visceral Leishmaniasis (VL), is a severe health issue in India, accounting for 18% of the global burden of the disease in 2020. The disease is caused by protozoan parasites from the Leishmania species, transmitted to humans by the bite of an infected female phlebotomine sandfly. The disease is endemic in 75 countries across Asia, Africa, and the Americas, with India being a significant contributor.
As of December 2023, Kala Azar remains a substantial public health problem in India, particularly in 54 districts across four states — Bihar, Jharkhand, Uttar Pradesh, and West Bengal. Despite the challenges, India has made significant progress in combating the disease, with Kala Azar cases decreasing by 98% since the start of intensified activities in 1992.
Epidemiology
- Kala Azar is a major health problem in India, with an estimated 146,700 new cases per year as of 2012.
- The disease is endemic in 54 districts across four states — Bihar, Jharkhand, Uttar Pradesh, and West Bengal.
- Bihar is the most affected state, with more than 90% of the cases.
- Sporadic cases are also reported in other states including Assam, Gujarat, Himachal Pradesh, Jammu & Kashmir, Kerala, Madhya Pradesh, Haryana, Puducherry, Sikkim, Tamil Nadu, and Uttaranchal.
- The disease manifests cyclical patterns of incidence in rural and peri-urbanization settings.
- The disease is associated with poverty, and the population at risk for Kala Azar is among the poorest in the community and often poorly nourished.
Clinical Manifestations
- Kala Azar is a disease in which a parasite migrates to the internal organs such as the liver, spleen, and bone marrow.
- If left untreated, the disease almost always results in death.
- Signs and symptoms include fever, weight loss, fatigue, anemia, and substantial swelling of the liver and spleen.
- Asymptomatic Kala Azar occurs when someone has the infection but does not show symptoms.
- Post Kala-azar Dermal Leishmaniasis (PKDL) is a late cutaneous manifestation of VL, typically occurring after apparent cure of VL, but sometimes even without a prior history of VL in India.
Diagnosis
- The mainstay of diagnosis is the demonstration of Leishman-Donovan (LD) bodies using Geimsa or other Ramonowsky stains.
- Several immunological tests are now available and they are more sensitive and specific than the aldehyde test.
- Antibody-based tests such as the rK39-based immunochromatographic strip test and the direct agglutination test (DAT) are widely used for the diagnosis of VL.
- However, their major drawback is continued positivity both long after cure and in a high proportion of individuals living in endemic areas.
Treatment
- The treatment of Kala Azar is hampered by drug resistance.
- Newer drugs are available and so are new delivery systems.
- There have been many breakthroughs in the past decade in the treatment of Kala Azar in India, such as approval of oral miltefosine and paromomycin, single-dose treatment with liposomal amphotericin B and multidrug treatment.
Control and Elimination Efforts
- The Government of India launched a centrally sponsored Kala-azar Control Programme in the endemic states in 1990-91.
- The National Health Policy-2002 set the goal of Kala-azar elimination in India by the year 2010 which was revised to 2015.
- India signed a Tripartite Memorandum of Understanding (MoU) with Bangladesh and Nepal to achieve Kala-azar elimination from the South-East Asia Region (SEAR).
- The elimination is defined as reducing the annual incidence of Kala-azar to less than 1 case per 10,000 population at the sub-district (block PHCs) level in Bangladesh and India and at the district level in Nepal.
- The eradication of PKDL should be a priority within the current VL elimination program aimed at achieving a goal of less than 1 case per 10,000 in the population at the district or sub-district levels of VL endemic areas.
Way Forward
- Intensify awareness campaigns with the involvement of communities and community health volunteers.
- Improve access to care in at-risk population and other underprivileged sections of communities.
- Strengthen disease surveillance and reporting systems.
- Enhance research on disease prevention strategies, drug resistance, and treatment modalities.
- Prioritize the eradication of PKDL within the current VL elimination program.
Conclusion
Kala Azar remains a significant public health challenge in India, particularly in the states of Bihar, Jharkhand, Uttar Pradesh, and West Bengal. Despite the progress made in reducing the incidence of the disease, there is a need for continued efforts in disease surveillance, access to care, community awareness, and research. The eradication of PKDL should be a priority within the current VL elimination program. With concerted efforts, it is hoped that the goal of eliminating Kala Azar as a public health problem can be achieved in the near future.
If you like this post, please share your feedback in the comments section below so that we will upload more posts like this.